
In my previous article I identified that players who possess weakness within their groin muscles are more likely to develop groin injuries. With this in mind, it is important for physiotherapists and conditioning staff to firstly understand how to assess and or diagnose such deficits, and secondly which exercises should be given to players to address identified strength deficits.
READ MORE > Hamstring and groin injury risk factors
For those treating and conditioning individuals with groin pain there is a wide range of literature spanning etiology, diagnosis and exercise management 1-16. Before I delve into which exercises should be used, I feel that it is important to provide you the reader with some basic understanding about how groin muscle strength can be assessed and what can be done with the information that is gained from the muscle strength assessment.
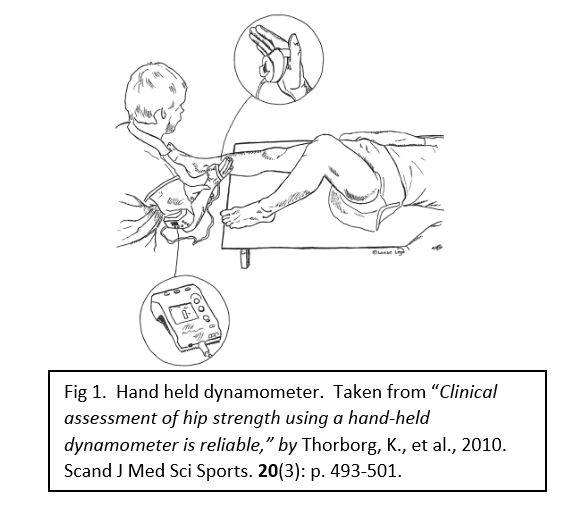
The known detrimental effects of groin weakness has led to the development of techniques to quantitatively and affordably assess groin muscle strength. Hand held dynamometry has gained popularity amongst physiotherapists, strength and conditioning staff and sports physicians in recent years as it provides an affordable and reliable way to assess groin strength17. A hand held dynamometer (HHD) provides the clinician with an understanding of the force that can be produced by muscles. It is a quick and easy way to determine deficits in muscle strength that are commonly missed in normal assessments. The sensor is placed against the leg of the participant and they are then asked to produce a maximal effort muscle contraction for a specified time period, usually between 3-5 seconds into the sensor (Fig1).
This can be used for all of the major hip muscle groups and allows for comparison between the different muscles around the hip and also between dominant and non-dominant limbs. When assessing hip strength with the HHD I am particularly interested in the balance between the hip adductors and hip abductors. These muscles should have identical strength and in some cases the hip adductors should be stronger than the hip abductors. It is known that the hip adductors should be at least 80% as strong as the hip abductors, this is thought to be the minimum strength level needed to protect against groin injury. If a player drops below this level he or she is at greater risk of injury.
Intuitively it could be assumed that all soccer players should have strong groin muscle given the nature of the sport, this could not be further from the truth. The list of causes for this imbalance is a mile long, but primarily I find that prior groin injury and/or inadequate conditioning practices that focus on sagittal plane strengthening over coronal plane exercise seem to be two common causes. The later makes sense, if you spend any time in gyms observing strength training behaviors, as the majority of individuals perform squats, lunges, dead lift and the like that are excellent for the posterior chain muscles but are unlikely to transfer develop muscle strength in the hip adductors.
Now onto exercises. Recent research10 has given us some nice understanding regarding which exercises produced sufficient muscle activity to provide a strengthening stimulus to the adductor muscles. Research into muscle exercises is primarily done with the aid of electromyography. This gives an idea of how much each exercise activates the specific muscles of interest, compared to a maximal contraction of that specific muscle.
European researchers provide us with the majority of scientific literature looking into groin pain in soccer players. Recently, eight commonly used exercises for groin rehab were investigated in order to find which exercise were the most effective for eliciting muscle activation in the hip adductors. 3 exercises stood out from the rest, firstly due to the greater muscle activation shown but also the ease of performance of each exercise10. The exercises are shown below:

Tweet at @JHeerey, @LaTrobeSEM, @FAI_Cohort and @mattgmking1 for more info
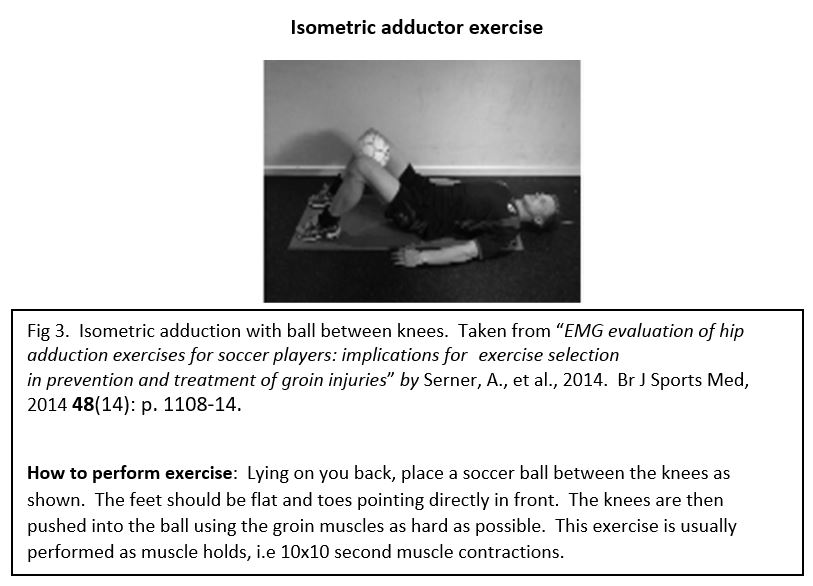
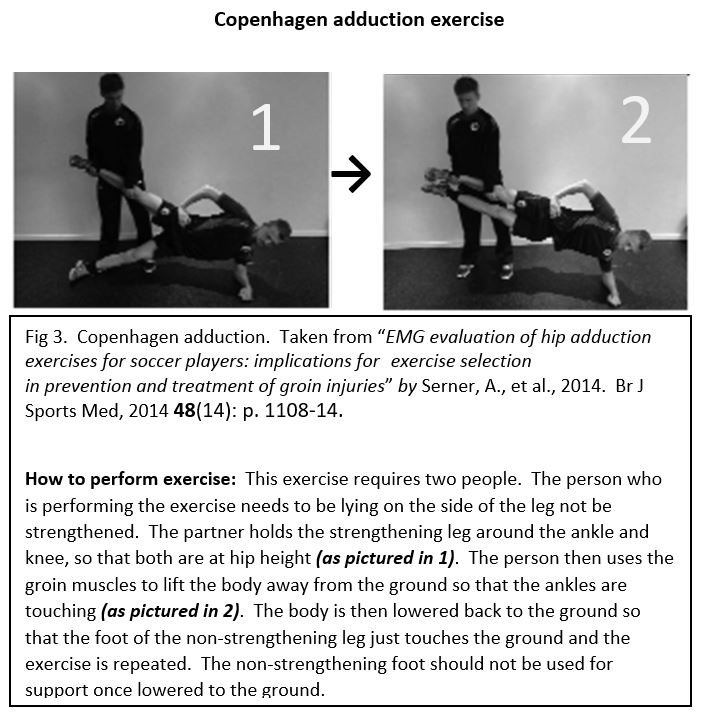
The great thing about all of the exercises is that they can be performed without the need for large pieces of expensive equipment. In particular the isometric adductor exercise and the Copenhagen adduction exercise can be performed on a pitch under the guidance of coaching or conditioning staff.
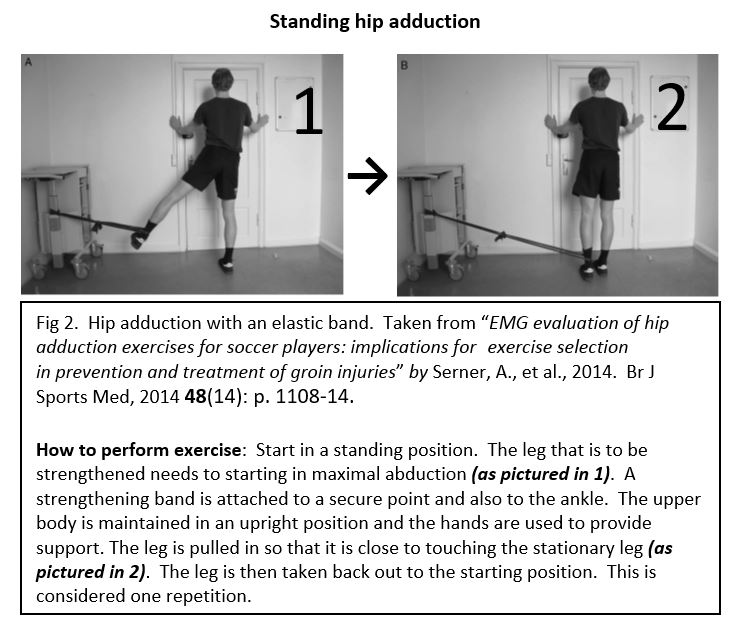
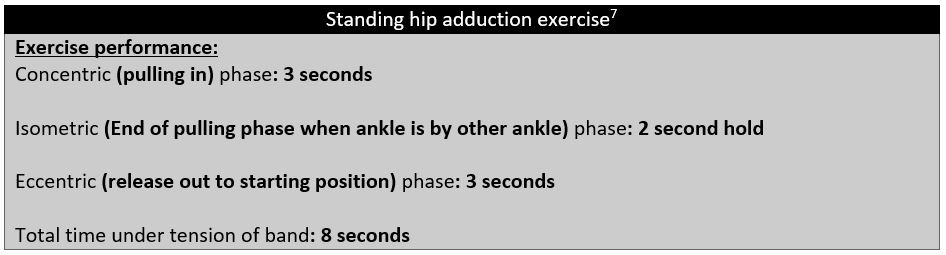
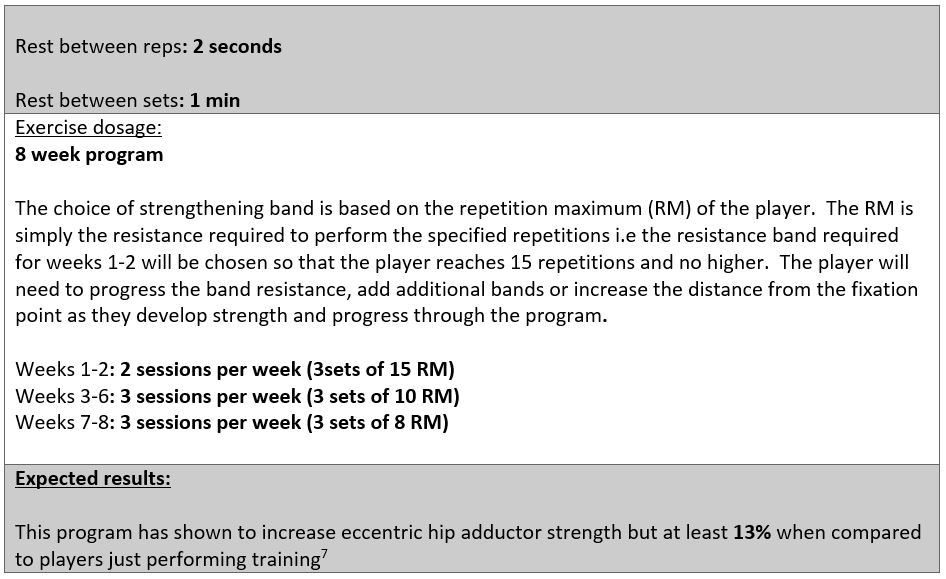
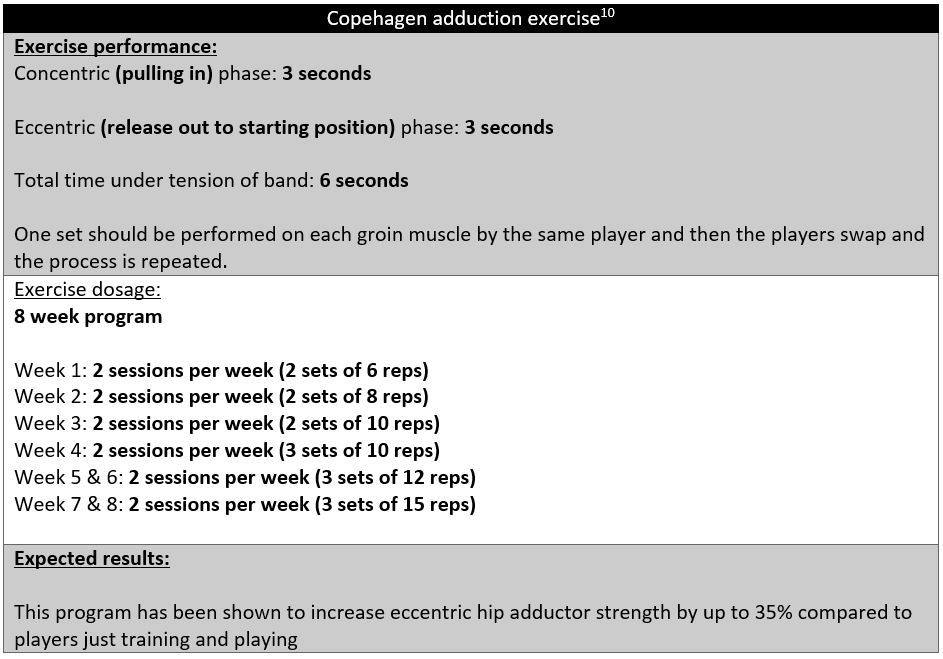
The question that is often asked is how many and how often should I perform the exercise. Luckily this has been covered for you as well, with the standing hip adduction and Copenhagen groin exercise being investigated in research7, 10. I have outlined how each exercise should be performed and the appropriate dosage and training period below:
In summary, management and prevention of groin injuries requires firstly appropriate strength assessment and secondly correct exercise prescription. The information above will hopefully provide physiotherapists, conditioning staff and players with an understanding of how groin injuries can be managed in a scientific evidence based way. Through adopting these proven methods the amount of groin injuries that a team will experience will be dramatically reduced.

A former Premiership winning player at South Hobart FC, Josh is a physiotherapist with extensive experience dealing with hip and groin pain in football players. He is currently undertaking his PhD, looking at hip and groin pain in soccer players. He consults privately at Clifton Hill Physiotherapy in Clifton Hill.
- Bradshaw, C.J., M. Bundy, and E. Falvey, The diagnosis of longstanding groin pain: a prospective clinical cohort study. Br J Sports Med, 2008. 42(10): p. 851-4.
- Branci, S., et al., MRI findings in soccer players with long-standing adductor-related groin pain and asymptomatic controls. Br J Sports Med, 2015. 49(10): p. 681-91.
- Esteve, E., et al., Prevention of groin injuries in sports: a systematic review with meta-analysis of randomised controlled trials. Br J Sports Med, 2015. 49(12): p. 785-91.
- Holmich, P., L.R. Holmich, and A.M. Bjerg, Clinical examination of athletes with groin pain: an intraobserver and interobserver reliability study. Br J Sports Med, 2004. 38(4): p. 446-51.
- Holmich, P., et al., Incidence and clinical presentation of groin injuries in sub-elite male soccer. Br J Sports Med, 2014. 48(16): p. 1245-50.
- Holmich, P., et al., Does bony hip morphology affect the outcome of treatment for patients with adductor-related groin pain? Outcome 10 years after baseline assessment. Br J Sports Med, 2014. 48(16): p. 1240-4.
- Jensen, J., et al., Eccentric strengthening effect of hip-adductor training with elastic bands in soccer players: a randomised controlled trial. Br J Sports Med, 2014. 48(4): p. 332-8.
- Maffey, L., Do the short-term benefits of physical training for sport-related groin injuries persist? Clin J Sport Med, 2012. 22(6): p. 522-3.
- Orchard, J.W., Men at higher risk of groin injuries in elite team sports: a systematic review. Br J Sports Med, 2015. 49(12): p. 798-802.
- Serner, A., et al., EMG evaluation of hip adduction exercises for soccer players: implications for exercise selection in prevention and treatment of groin injuries. Br J Sports Med, 2014. 48(14): p. 1108-14.
- Sheen, A.J., et al., ‘Treatment of the sportsman’s groin’: British Hernia Society’s 2014 position statement based on the Manchester Consensus Conference. Br J Sports Med, 2014. 48(14): p. 1079-87.
- Thorborg, K., et al., Eccentric and Isometric Hip Adduction Strength in Male Soccer Players With and Without Adductor-Related Groin Pain: An Assessor-Blinded Comparison. Orthop J Sports Med, 2014. 2(2): p. 2325967114521778.
- Thorborg, K., et al., Hip adduction and abduction strength profiles in elite soccer players: implications for clinical evaluation of hip adductor muscle recovery after injury. Am J Sports Med, 2011. 39(1): p. 121-6.
- Weir, A., et al., Doha agreement meeting on terminology and definitions in groin pain in athletes. Br J Sports Med, 2015. 49(12): p. 768-74.
- Weir, A., et al., Terminology and definitions on groin pain in athletes: building agreement using a short Delphi method. Br J Sports Med, 2015. 49(12): p. 825-7.
- Weir, A., et al., Manual or exercise therapy for long-standing adductor-related groin pain: a randomised controlled clinical trial. Man Ther, 2011. 16(2): p. 148-54.
- Thorborg, K., et al., Clinical assessment of hip strength using a hand-held dynamometer is reliable. Scand J Med Sci Sports, 2010. 20(3): p. 493-501.